
Julian Perez, J.D., Chief Legal Officer, dentalcorp
Most dentists prefer to avoid lawsuits, regulatory complaints, medical emergencies, or for that matter, any clinical adverse events. Such incidents, at a minimum, cause stress, consume time, and erode profits. At worst, adverse events morph into traumatic career-altering experiences. Fortunately, there is a tried-and-true antidote that helps clinicians prevent and mitigate such unfortunate events: i.e., the medical history Form.
If you view medical history forms as a paperwork problem, bear with me. It’s true that clinical charting isn’t as exciting as artificial intelligence or 3D printing; however, perhaps that should change. A decade in dental regulation, malpractice and risk management has made clear that the importance of medical history forms and processes is paramount. Indeed, if any single document in your office has the power to save a life, that document is one of your patient’s medical history forms (and hopefully the medical alert set up in response to the information disclosed there). Consider a few of the most common medical emergencies that occur in dental offices: excessive bleeding, adverse drug reactions, anaphylaxis, syncope, epileptic seizure, cardiac arrest, acute asthma attack, and diabetic emergencies.[1]
If not managed properly, any one of these conditions can result in serious harm, liability, stress and regret. If one of your patients is at risk for a serious adverse outcome, wouldn’t you want to know? And if one of your dental assistants suffered a percutaneous exposure from a contaminated instrument, wouldn’t they want to know if the patient they were treating carried any bloodborne pathogens? In both cases, the desired information ought to be found in the medical history form.
Medical histories are more important today than ever.
Both you and I know, unfortunately, there’s a good chance the information in tomorrow’s medically complex patient’s chart is either out of date, incomplete, hard to access, incorrect or otherwise lacking. Yet, medical histories have never been more vital in reducing risk: “Medical complications during dental treatment are increasingly anticipated because advances in medical treatment have prolonged life expectancy.”[2] At the same time, “[t]he demands for patients to undergo invasive dental treatment, for example, implantology or periodontal surgery, has increased.”[3]
Most patient safety incidents in the dental office are minor (or very minor); however, that is not always the case. A study in the UK uncovered 120 deaths in dental practices over the last 10 years. Similarly, in the Netherlands, the patient charts of 288 dentists were reviewed. The investigation found that 208 emergencies were reported in a 1-year period, including one sudden death due to myocardial infarction.[4] This means that dentists may expect one medical emergency every 16 months on average. While the message is sobering, the truth is unavoidable: the risk of harm in dental clinics is increasing as the population ages and invasive surgeries increase.
Having an accurate medical history is the beginning, not the end.
Addressing this inevitable demographic trend necessitates clinical flexibility, broader awareness of relevant conditions and expertise in the side effects and interactions of various medications. When a medically complex patient presents with a chief complaint that calls for an invasive procedure, the dentist will have to consider various treatment planning factors that might be taken for granted in healthy individuals. Figure 1 from an article by Cathy Bryant, et al., demonstrates an array of factors a clinician should weigh when treatment planning for a medically complex patient. These factors are above and beyond the usual considerations:
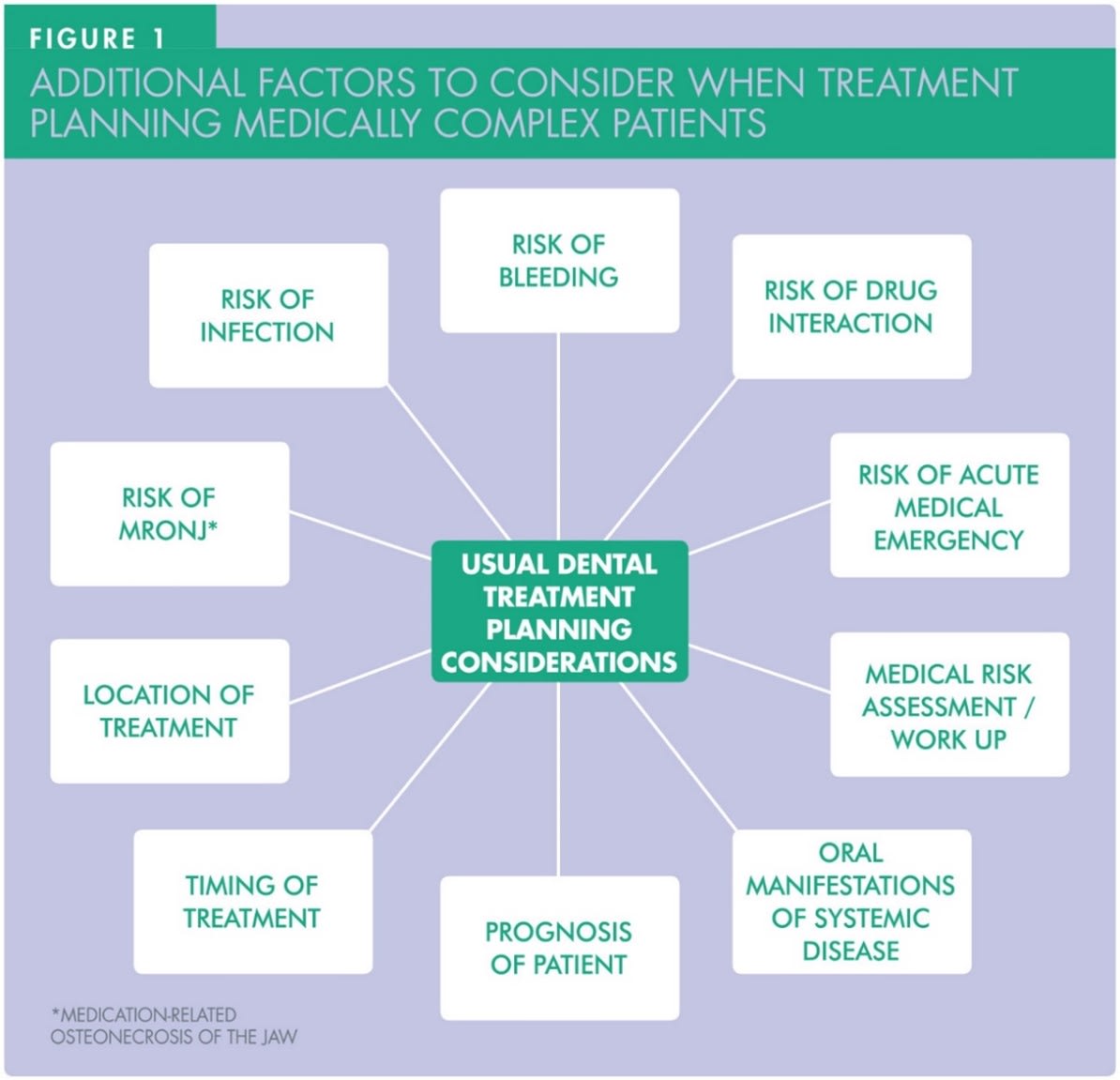
[5]
Don’t expect patients to fill out the form correctly.
Establishing a process likely to generate reliable information requires understanding how patients behave. If you think that patients will generally fill out medical history forms correctly, you’re wrong. If you think patients are likely to at least include important past health information, think again. Let’s consider, by way of example, patients who receive direct oral anticoagulants (DOACs). Not only is the number of patients taking such drugs increasing, but the treatment is also associated with a heightened risk of bleeding; moreover, hemorrhage after tooth extraction in patients on DOACs is frequent with an incidence up to 26% and may range from minor to life threatening.[6]
Considering this fact, dental researchers set out to see how many patients taking bisphosphonates included that information on their medical history forms prior to dental care. To do this, Volong Dao, D.M.D, et al. reviewed charts of 112 patients to determine what percentage had included bisphosphonate use in their health history form. The findings were startling: “Only 35% of our patients who were using bisphosphonates had reported taking bisphosphonates on the health history form.”[7]
There are several reasons why patients might fail to include such critical health information. First, patients may not be accurate when answering a health questionnaire (in the dental office) because they do not understand which, if any, medical conditions might be relevant to dental care. Patients may also be in a rush, have low literacy or health literacy, or feel embarrassed to disclose certain information. One qualitative study that looked at this question concluded that “disclosure behavior can be affected by age, history of diagnosis, history of disclosure, professionalism of dentists, and knowledge and presence of oral effects.”[8]
The good news is there are lots of strategies to improve.
Phenomena in the greater healthcare system have implications for dentistry. The fact that many areas of Canada currently face shortages in family physicians makes dentists more likely to encounter patients with no primary care provider. As a result, patients may present with significant undetected risk factors (e.g., hypertension) or know about conditions that have become uncontrolled (e.g., diabetes).
While each patient and situation are unique, there are actions dentists can take to mitigate risk and provide better quality care to their patients. Such steps include:
- Taking the patient’s vitals and documenting findings, such as blood pressure and pulse.
- Recording the patient’s self-evaluation and objective condition in the chart notes.
- Assisting the patient in finding a family physician.
- Including specific language about the risks of receiving dental treatment without full knowledge about overall health in informed consent to treatment documents.
- Advising the patient that non-urgent or invasive dental treatment must be delayed until health information is gathered, or the specific condition is managed.
- Ensuring after care calls are made to patients who underwent oral surgery.
- Following up with the patient to request confirmation that they have seen a physician.[9]
When considering risks that may manifest secondary to dental treatment, keep in mind that emergencies may present immediately in the clinic or, as in the case of an adverse drug reaction or excessive bleeding, after the completion of treatment when the patient has been discharged. To prevent such emergencies from escalating, following up with patients after an invasive procedure is good practice.
Conclusion
Past medical history is an essential component of a dentist’s risk assessment for the likelihood of a patient experiencing a medical emergency. [10] When thinking about medical history, it’s essential to consider both the content of the medical history form as well as the processes employed when obtaining a history. Ensuring the accuracy of your patients’ records is not a paperwork problem, it demands that dental teams understand and implement the use of good communication skills. Dentists need to get to know their patients and not expect that patients will automatically or invariably disclose important information. That information may have to be coaxed out through open ended questioning and conversation. With that in mind, the objectives for the history-taking part of any new patient exam or subsequent dental consultation are (1) to foster an effective dentist-patient relationship, and (2) to obtain an accurate and comprehensive picture of the patient’s relevant medical history and condition.
If you’re still not convinced about the importance of excellence in medical history taking, it’s technically the law. The guidance from the regulatory body in Ontario says it all, “The patient’s medical information should be reviewed and updated regularly to ensure that it remains accurate.”[11] If you just follow this rule, you’ll have more satisfied patients and fewer unpleasant surprises!
Originally published in Oral Health journal.
[1] Dealing with the most frequent medical emergencies in the dental office, available at https://oasisdiscussions.ca/2014/08/22/de/. Based on General medicine and surgery for dental practitioners: part 3, M. Greenwood and J. G. Meechan, BDJ, August 2014.
[2] Psychometric Analysis of the European Medical Risk‑Related History Questionnaire within Indonesian‑Speaking Population, Yuniardini Septorini Wimardhani, et al., Jour of Int’l Soc of Preventive & Community Dentistry, 2019. [3] Id.
[4] Id. [5] Oral surgery: Considerations for the medically complex patient, Cathy Bryant, et al., Primary Dental Journal, September 2022; available at https://journals.sagepub.com/doi/epub/10.1177/20501684221112493. Last accessed January 10, 2023. [6] Severe Enoral Bleeding with a Direct Oral Anticoagulant after Tooth Extraction and Heparin Bridging Treatment, Case Rep Emerg Med., Simone Ehrhard, et al., 2019; available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6875271/#:~:text=Excessive%20bleeding%20is%20a%20risk,to%20life%20threatening%20%5B3%5D. Last accessed January 9, 2023. [7] Bisphosphonate Use and Health History Questionnaire, Volong Dao, D.M.D.; Richard A. Kraut, D.D.S., NYSDJ • NOV 2008. [8] Why individuals with HIV or diabetes do not disclose their medical history to the dentist: a qualitative analysis, J. Edwards, G. Palmer, N. Osbourne and S. Scambler, BDJ, 2013. [9] Medical/Dental Health History, Guidelines for Practice Success | Managing Professional Risks | Patient Records, Charting, and Documentation Protocols, ADA; available at https://www.ada.org/resources/practice/practice-management/medical-dental-health-history. Last accessed on January 10, 2023. [10] Essentials of Medical History Taking in Dental Patients, Mark Greenwood, PhD, MDS, DentUpdate, May 2015. [11] Medical History Recordkeeping, A Guide for Ontario Dentists and Their Patients, RCDSO, available at: https://az184419.vo.msecnd.net/rcdso/pdf/medical-history-recordkeeping/RCDSO_Medical_History_Recordkeeping_Guide.pdf, last viewed January 9, 2023.
